VOL. 23, No. 3, 75 - 96
We report here on an exploratory formative evaluation of a project to integrate mobile learning into a Western Canadian college nursing program. Third-year students used Hewlett Packard iPAQ mobile devices for five weeks in a practice education course in April - May, 2007. Koole's (2009) Framework for the Rational Analysis of Mobile Education (FRAME) model provided our definition of mobile learning and was used to organize our presentation of the results of the study. Participants reported positively on the usability of the mobile devices, finding them easy to learn, readily portable, and the screen size sufficient for mobile specific programs. However, they had difficulty with the wireless connectivity and, despite an initial orientation, did not have time to fully learn the devices in the context of a busy course. As a result, it is not clear if students can effectively use the social technology provided by such devices or if mobile learning can support interaction between instructors and learners in this context. The use of mobile devices in nursing practice education is feasible, but further investigation is needed on the use of m-learning for communication and interactive purposes.
Nous faisons ici état d’une évaluation formative exploratoire d’un projet visant à intégrer l’apprentissage électronique sans fil dans un programme de sciences infirmières du collège Western Canadian. Des étudiants de troisième année ont utilisé des appareils sans fil Hewlett Packard iPAQ pendant cinq semaines dans le cadre d’un cours d’éducation pratique en avril-mai, 2007. Le modèle (2009) FRAME (Framework for the Rational Analysis of Mobile Education) de Koole (2009) a fourni notre définition de l’apprentissage électronique sans fil et a été utilisé pour organiser notre présentation des résultats de l’étude. Les participants ont fait un rapport positif sur la facilité d’emploi des appareils sans fil, trouvant qu’il était facile d’apprendre à les utiliser, qu’ils étaient faciles à transporter, et que la taille de l’écran était suffisante pour des programmes conçus pour ces appareils sans fil. Toutefois, ils ont eu de la difficulté avec la connectivité sans fil et, malgré une formation initiale, ils n’ont pas eu le temps de pleinement apprendre le fonctionnement des appareils dans le cadre d’un cours chargé. Il en découle donc, qu’il n’est pas certain que des étudiants puissent effectivement utiliser la technologie sociale offerte par de tels appareils ni que l’apprentissage électronique sans fil peut soutenir l’interaction entre les enseignants et les étudiants dans un tel contexte. L’utilisation d’appareils électroniques sans fil est possible, mais des enquêtes plus poussées sont nécessaires sur l’usage de l’enseignement électronique sans fil pour des fins de communication et interactives.
In modern healthcare, practitioners are pressured to manage the high acuity of their patients' health challenges and an increasing pace of practice in addition to coping with an explosion of knowledge and technology. Practitioners are forced to access and process clinical data efficiently by drawing on current resources to support safe care and evidence-informed practice at the point-of-care. Moreover, client care is increasingly shifting to the community, an environment where resources are not readily accessible (Villeneuve & MacDonald, 2006).
These ongoing changes are also influencing models of Nursing practice education. Increasingly, indirect supervision models are used as Nursing Education programs admit more students to address the nursing shortage and as students are placed in community and other non-traditional clinical practice environments. Although modern communications technologies might assist to decrease student isolation, students are often unable to access these technologies in the practice setting. In addition, supervising nurses are facing increasing workloads and find it challenging to also supervise student nurses. This is compounded by decreased peer and instructor communication with the result that students are left more isolated in practice.
New approaches and tools to support the teaching and learning of nursing students at a distance are needed and mobile learning (m-learning) is one possible response. M-learning has the potential to bring the instructor, peers and resources together virtually at the point-of- care, especially when indirect supervision models are used, to support the students' safety and evidence-informed practice.
Mobile Learning Defined
Traxler (2007) defines m-learning as the personalised, connected, and interactive use of handheld computers in classrooms, in collaborative learning during fieldwork, and in counselling and guidance. It supports learning that is more situated, experiential and contextualized within specific domains and affords the creation and use of up-to-date and authentic content (Kukulska-Hulme & Traxler, 2005).
As a result, m-learning can readily be applied in distance or blended learning contexts. Keegan (1996), for instance, defines distance education as characterized by the quasi-permanent [emphasis added] separation of teacher and learner throughout the length of the learning process and involving two-way communications so that the student may benefit from, or even initiate, dialogue (p. 50). Similarly, Garrison and Kanuka (2004) define blended learning as "the thoughtful integration of classroom face-to-face learning experiences with online learning experiences" (p. 96) [emphasis added]. By online learning, they mean the use of asynchronous Internet communication technology to facilitate learning experiences that allow learners to be independent of space and time and yet together in order to foster a community of inquiry (p. 97). Current mobile technologies such as smart phones and personal data assistant (PDA) style mini-computers can readily provide both asynchronous and synchronous two way communications to foster educational dialogue at a distance. We were especially interested in these capabilities for indirect nursing supervision contexts.
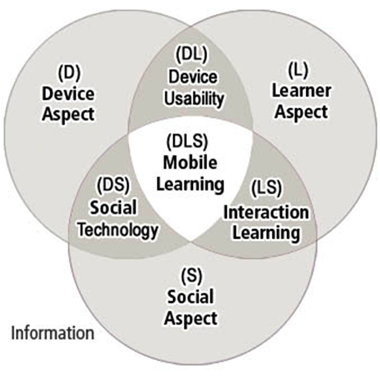
The FRAME Model. We found Traxler's definition of m-learning insufficient to guide our investigation in Nursing Education (Kenny, Park, Van Neste-Kenny, Burton, P.A. & Meiers, 2008, 2009) and turned to Koole's Framework for the Rational Analysis of Mobile Education (FRAME) model instead (Koole, 2005, 2009; Koole & Ally, 2006) (See Figure 1). Koole defines m-learning as a process resulting from the interaction of mobile technologies, human learning capacities, and the social aspects of learning.
Figure 1. Koole's FRAME model (used
with permission of the author)
The Device Aspect of the model focuses on the physical and functional components of mobile devices, i.e., the medium through which learners interact and which impacts their physical and psychological comfort levels. The Learner Aspect refers to the individual learner's cognitive abilities and prior knowledge, while the Social Aspect describes the social context for learning.
While these main aspects are clearly important, we believe that it is the interactions between them that are most likely to determine the effectiveness of m-learning. These interactions are represented in the intersections as device usability, social technology, and interaction learning. Device Usability relates the characteristics of mobile devices to cognitive tasks and the manipulation and storage of information, while Social Technology describes how mobile devices enable communication and collaboration. Interaction Learning focuses on the social interaction that social technology enables. In an m-learning context, the software applications (e.g., text messaging, email or audio conferencing) provided by mobile technologies constitutes the social technology. These applications in turn may allow learners to interact in learning communities where they can acquire information and negotiate meaning. The ensemble of these components then defines the m-learning process.
Mobile Learning in Nursing and Nursing Education
Nurse practitioners use PDAs for many reasons, including to keep task lists, as memo pads, calculators, expense trackers, calendar/date books, patient manager, clinical reference material, address/phone book, information exchange, e-mail and Internet access (Cahoon, 2002; Rosenthal, 2003; Stroud, Erkel, & Smith, 2005). Newbold (2003) adds such clinical applications as ordering test results, keeping patient histories, progress notes and assessments, and searching for references, protocols, and prescription information. Nurses also employ PDAs in practice because they are light, convenient, lead to fewer medication errors (when nurses use drug reference software instead of relying on memory), allow access to the Internet, and are used to explore options with clients (Davenport, 2004; Park, 2006).
In nursing education, instructors use mobile devices to keep records of student assignments and checklists for completing physical assessments, as a source of point-of-care reference (drug software) and to document student progress on-the-spot (Lehman, 2003). Goldsworthy, Lawrence and Goodman (2006) reported a significant increase in self-efficacy among student nurses when using PDAs in administering medications, while Miller et al. (2005) found students utilizing such devices had increasing numbers of questions in the practice setting, as well as a greater recognition of the need to use current resources.
Nursing Education and the FRAME Model
As discussed above, research on nurses' use of PDAs has focused mainly on device usability (Cahoon, 2002; Newbolt, 2003; Rosenthal, 2003) and shows they are early adopters of PDAs for resource purposes. The social technology and interaction aspects are virtually unexplored in the research literature and it is these aspects of mobile devices that afford mobile distance education and blended learning. Students mainly mention the use of email to communicate with others via PDAs (Stroud et. al., 2005; Park, 2006). There has been little research on the use of mobile devices for social interaction among health care professionals and the potential of mobile devices to provide connectivity in teaching and learning has not been explored (Kenny et al., 2009). M-learning may afford learners immediate and ongoing access to information, to peers, and to instructors and other experts who can help them determine the value of information found on the Internet and in their real-world environments. The research reported in this paper focuses on an initial, exploratory study of these possibilities within the context of Nursing practice education and sets the results in the context of the FRAME model (Koole, 2005, 2009).
This study was part of a two-stage formative evaluation of the use of mobile devices in Nursing practice education. Stage 1, a one-on-one trial with 2 instructors and 3 fourth-year students in a Baccalaureate Nursing (BSN) Program at a western Canadian community college, tested the feasibility of m-learning with nursing students before their introduction into live instruction and is reported in Kenny et al. (2009). This paper discusses the results of Stage 2, in which we conducted a full field trial of mobile learning in a real-life nursing practice education course at the same institution.
Research Setting
In Stage 2, we used mobile devices in a nursing practice education course taught at the end of third year. This class, held in April - May, 2007, was a practice consolidation experience of 5 weeks in duration and was taught by the 2 instructors who participated in Stage 1. The course is best described as a form of blended learning (Garrison & Kanuka, 2004). The students first met with the instructors in an initial face-to-face class and then attended assigned, off campus, hospital and community placements for the duration. The instructors did not directly supervise their students in these experiences. Rather, they either met each student in person or telephoned them at certain intervals. This contact varied with the instructor, but at most, took place once a week at the end of every set of 12-hour shifts. All other activities, including online discussions in WebCT, and text and voice communications using the mobile devices, were conducted at a distance.
Seventeen of the 22 students in the course, including all 3 students asking for community placements, volunteered for the study. Since we had an insufficient number of devices for all participants, wee assigned them to 2 groups: a mobile learning (m-learning) group of 12 students and a comparison group of 5 students. The groups were selected using both purposive and random stratified sampling. We expected that the mobile devices would be especially important for maintaining communications with students in community settings, since they were assigned individually to these placements and would have contact with fewer practising nurses and fellow students than those in the hospital settings. To achieve as much balance as possible between clinical settings, we assigned all 3 students in community placements to the m-learning group and randomly selected the other 9 m-learning students from the 14 volunteers placed in 2 local hospitals. The remaining volunteers were asked to participate in the comparison group. While not intended as a true control group in experimental terms, this group allowed us to compare the post survey responses of our mobile learning group with similar students not using the devices.
Mobile Devices
The m-learning group members were each provided with a Hewlett-Packard iPAQ Model 6955, an integrated pocket PC computer, mobile telephone and digital camera, that provides both WiFi and GPRS wireless connectivity for voice and data download. This model used Windows Mobile 6.0 and included Microsoft (MS) Office, Internet Explorer and Pocket MSN Messenger. As well, we provided the 2007 Lippincott Nursing Drug Guide, the Davis Lab and Diagnostic Tests, the Skype audio conferencing program, and Adobe Acrobat Reader Mobile.
Study Design
The purpose of this study was to evaluate whether the implementation of mobile devices in an independent nursing practice education setting would be feasible and practical, and to assess if nursing students and instructors would find the use of such devices in this context to be comfortable and helpful in assisting their learning.
Stage 2 was a full field trial. Field trial evaluation should be conducted in actual situations that contain all of the elements of the learning environment Tessmer (1993). We tested the use of the mobile devices in Nursing 357, a nursing practice education course that is an integral part of the four-year BSN curriculum. Several forms of evaluation data were collected in this study:
The pre-study demographic survey was tallied and descriptive statistics compiled. The interviews were transcribed and coded using AtlasTi. Each interview was coded by two research team members independently and the codes were merged. The final codes were negotiated by the research team and consolidated codes were grouped into networks or themes.
Here, we report the findings in the context of the FRAME model (Koole, 2005, 2009). Since the device and social aspects of the model were reviewed above in terms of the characteristics of the devices used in the study and the study context, we begin with learner demographics (the Learner Aspect) and then focus on the interactions between the main aspects as represented in the intersections: device usability, social technology, and interaction learning.
Learner Aspect
The Learner Aspect focuses on those cognitive abilities and prior knowledge which a learner needs to succeed in a specific context. In this study, we examined our participants' comfort with both desktop computing and mobile devices and their prior experience with mobile devices. Table 1 reports the age ranges and gender of our participants. They were predominantly female and heterogeneous in age.
Table 1. Age and Gender of the Participants.
Age Range |
Mobile Group (N = 12) |
Comparison Group (N = 5) |
Total |
18 - 25 |
3 |
1 |
4 |
26 - 29 |
2 |
2 |
4 |
30 - 39 |
5 |
1 |
6 |
40 - 49 |
2 |
1 |
3 |
Gender |
|||
Female |
11 |
4 |
15 |
Male |
1 |
1 |
2 |
Prior knowledge of computing and of mobile devices. The survey data and interviews revealed that most of our participants felt quite comfortable with personal computing (See Table 2). All had owned a personal computer for at least 2 years prior to the study and all used the Microsoft Windows operating system.
Table 2. Participants' Level of Comfort with Computing.
Prior Level of Comfort |
Desktop (N = 17) |
Mobile (N = 15) |
| Very uncomfortable | 0 |
0 |
| Somewhat uncomfortable | 0 |
4 |
| Somewhat comfortable | 8 |
8 |
| Very uncomfortable | 9 |
3 |
Note: Two participants did not answer the question about comfort with mobile devices.
None reported discomfort with desktop computing. Their experience with m-learning, on the other hand, was limited. Thirteen participants owned mobile phones and 6 of these had a smart phone. For most of the participants, however, this was their first experience with a PDA - style pocket computer, that is, one that used the MS Windows Mobile desktop and applications. They had all used MS Windows, MSOffice, and Hotmail on desktop computers, but not on pocket computers. Some had seen nursing software for PDAs demonstrated, but none had used it in practice.
Regardless, the 11 participants who responded to the question reported that they were at least somewhat comfortable with PDAs. This was surprising since their prior experience clearly was mainly with mobile telephones and digital cameras built into their mobile phones. Some were also familiar with traditional PDA functions such as task lists and calendars, but not with the range of functions and software provided in the HP iPAQs (See Table 3). The interviews, however, revealed that this comfort was largely based on their experience with desktop computing rather than as a result of the specific applications on mobile devices. Terrie's1 response exemplifies this:
Well, I have a fee… being comfortable on a computer is a good start, because… to me it's a little version of a computer, right? Especially with the Windows program and such. If you're comfortable on a computer and how to search the internet… different addresses and just how to do a basic search… you would need that sort of knowledge.
Table 3. Prior Experience with Mobile Devices.
Feature |
None |
Beginner |
Competent |
Experienced |
N |
| Telephone | 2 |
2 |
4 |
7 |
15 |
| Photography | 5 |
3 |
5 |
2 |
15 |
7 |
3 |
3 |
2 |
15 |
|
| Internet | 6 |
5 |
2 |
2 |
15 |
| Text Messaging | 6 |
1 |
6 |
2 |
15 |
| Audio Messaging | 9 |
2 |
2 |
2 |
15 |
| Word Processing | 9 |
3 |
1 |
2 |
15 |
| Spreadsheet | 10 |
3 |
1 |
1 |
15 |
| Database | 10 |
3 |
1 |
1 |
15 |
| Nursing Software | 9 |
2 |
1 |
1 |
15 |
Note: N = 15. Two participants did not complete this part of the survey.
In summary, it appears that our participants had both the pre-disposition and prior knowledge to engage in mobile learning in this context. They uniformly reported being comfortable, if not completely familiar, with mobile technologies and interested in their application to their learning. However, as we will report below under the section on device usability, this positive disposition did not completely translate to effective learning of the iPAQ applications.
Device Usability
Device usability relates the characteristics of mobile devices to their application in cognitive learning. In our study, we first assessed how easily and how well our participants learned to use the applications and features of the iPAQ mobile devices. We then focused on their use of the devices in their learning and evaluated their assessments of both ease of use and any barriers to use that they perceived.
Learning the mobile device features. It was not simple for our participants to learn to use all the features available on these devices. They had access to a wide range of software and a variety of built-in features and accessories, including three different keyboards: a touch screen keyboard, a thumbing keyboard, and a full sized, detachable, folding keyboard. In addition, our participants could use either WiFi hotspots or General Packet Radio Service (GPRS) wireless connectivity for text messaging, to send email, to browse the Internet, or to use an audio conferencing program (e.g., Pocket MSN Messenger or Skype). For the study, the iPAQs were set up with local area service GPRS connectivity and WiFi was available on campus and in spots around the community (e.g., coffee shops) as well as the home networks of some participants.
We provided the mobile learning group with a 2-hour orientation to the devices at the beginning of the study, where we presented a number of features and provided time to practice under supervision. They were introduced to: a) the use of both the touch and thumbing keyboards, b) handwriting to text transcription, c) enabling wireless connectivity (WiFi and GPRS) for email and Internet browsing, d) the use of the nursing drug and lab values software, and e) the use of text and audio messaging (Skype). Any further instruction was done by individual request to the instructors. No technical support was provided by the college. In fact, our interviewees indicated that they felt no need for technical support beyond that provided by the instructors nor did they require more training. Instead, they referred to the user manual provided or learned how to use the application on their own. A comment from May exemplified this attitude:
Mmmm. Well the orientation session was really helpful. Uh… in learning how to use it. That basically answered pretty much all of my questions on… on learning to use the device. Other things… I didn't really encounter too many problems. Other things I just kind of figured out from trial and error …
Table 4 reports the mobile group participants' post-survey views on the ease of learning the various mobile applications. Curiously, while participants mostly reported that the mobile applications were easy to learn, the usage data showed that participants engaged in minimal use of GPRS connectivity to download data.
Table 4. Ease or Difficulty Learning the Mobile Applications.
Application |
Very Difficult |
Difficult |
Relatively Easy |
Easy |
N |
| Telephone | 0 |
0 |
4 |
8 |
12 |
1 |
0 |
5 |
5 |
11 |
|
| Browsing Internet | 0 |
0 |
6 |
6 |
12 |
| Text Messaging | 2 |
0 |
7 |
3 |
12 |
| Audio Messaging | 3 |
4 |
4 |
1 |
12 |
| Pocket Word | 1 |
1 |
4 |
6 |
12 |
| Pocket Excel | 2 |
1 |
4 |
4 |
11 |
| Drug Software | 0 |
0 |
5 |
7 |
12 |
| Lab Software | 0 |
1 |
5 |
6 |
12 |
Note: Two participants omitted questions in this part of the survey.
Only 2 of the 12 mobile group members downloaded more than 10 MB of data over the 5 weeks. The rest used 2 MB or less and most (8 students) did not use this feature at all.
Clearly, most did not use the devices to access the Internet or send email while they were in their practice experiences. One likely reason was that neither hospital nor any of the other placements where they were assigned had WiFi hotspots. One hospital did have WiFi in the cafeteria, but not on the wards. GPRS connectivity, therefore, would have been the most likely way for them to use these applications in practice.
When asked in the interviews about how well they learned to use the mobile devices, participants raised two main concerns. First, most students found that the intense nature of the one-month practice experience left them with insufficient time to focus on mastering the devices and, therefore, they tended to use them less than they might otherwise have done. It was a voluntary, not required, learning activity. Joan explained this issue:
I thought it was really very neat and I... I feel a little bit bad that only in the last couple of weeks just started getting in to it more. I think I was really quite overwhelmed with everything else getting started and it was really busy where I was, so I wasn't utilizing it as much, so I had um… not remembered everything that I had sort of learned, so it took a little bit more to start learning things. But the last couple of weeks I really started using it a lot more and started to enjoy… and not feel afraid of it.
The second issue was that, because the students did not own the devices, they felt less inclined to invest time in learning to use them and were afraid to damage what they viewed as expensive devices. Joan also noted that:
I think a longer period of time would have loaned itself well… just to the fact that you needed that… okay, like putting everything into the calendar, for instance. Right, well you spend this time loading it all in and it's only for this amount of time and as it was, you know, our time was very, very limited, short with things. You know, in terms of assignments and clinical and doing extra things and...
Ease of Use. Despite the apparent complexity of the devices, our participants uniformly claimed these devices were easy to master overall. After the orientation, they found they only required a few hours learning on their own to become proficient with the iPAQs. In the post survey, nearly 78% of the mobile group responded that it that it took them one-hour or less to learn individual applications.
Portability. One of the most pervasive arguments for mobile learning is that mobile devices are easily carried. Our participants generally agreed that the iPAQs were portable, but some found them heavy to attach to their uniforms. Joan's comment is representative of how the devices were carried:
It was fairly portable. I mean, because I had my big bag with me and it also fit in my purse too, so I could actually take it with the… uh… if I was leaving the office and I didn't take my big school bag I could pop it in my purse or take it with me when we were going to see clients or clipped on too… most of my of my clothing it clipped on okay, but if I was wearing a skirt that was a little bit thinner and it would pull it down a little bit right? I would feel uncomfortable wearing it, it was better when I had jeans on. Like, something that was a little bit more heavier weight to it.
Screen Size. Kukulska-Hulme and Traxler (2005) considered mobile technologies useful to support more situated learning. However, this implies that users can comfortably and effectively use their mobile devices for the task at hand. Our respondents pointed out that the iPAQ screens were too small for many learning tasks. They found them acceptable when using mobile formatted programs such as the drug reference program, but not when they had to scroll both vertically and horizontally when browsing non mobile formatted web sites or reading or creating word processing documents. Alice, for example, commented:
Um… I found that it was great, like as far as looking up, um, the drugs or the procedures or IV… procedures or what not. But um, for Word documents, I found, without the keyboard, the screen… it was very difficult with the small screen to type an actual full Word document.
Barriers to Use. The most difficult feature to use for participants was wireless connectivity. Despite orientation, few participants appeared able to make the GPRS data connection work when using the devices on their own. Our participants also talked about their inability to use wireless connectivity in the hospital. At the time of the study, local hospitals in our region did not allow the use of wireless devices on the premises for fear of causing medical equipment to malfunction and, therefore, neither supplied WiFi connectivity nor allowed the use of GPRS devices at the bedside. Terrie commented on the inconvenience and her resultant choice not to use her mobile device connectivity in practice:
Terrie: I couldn't have the Internet on in my practice for some reason… I just left it off because I didn't know what the issues were… with that, and I… and I couldn't access... I tried to get on to it at the [local area] hospital, I couldn't get internet on the… what's it? Hi-Fi?
Interviewer: WiFi.
Terrie: WiFi, yeah. I couldn't pick it up on my… well on my floor. I could in the cafeteria, but… so I didn't really use internet up there a lot.
Participants also could not use the iPAQs to access the WebCT course website that was the main vehicle for communications and for sharing of resources in the nursing practice course due to a JavaScript problem. This highlights the need for the use of LMSs and web sites that have been designed specifically for mobile use (e.g., Google Mobile). Joan's comment highlighted the problem:
And I guess it would have made it better had we been able to access WebCT, because that's where I was sending all my documents from home, right?
Social Technology — The iPAQ in Context
The Social Technology intersection describes how mobile devices enable communication and collaboration. In the context of this course, communication and collaboration would transpire between instructor and student or among students. Since the use of mobile devices for resource use is already well established (Kenny et al., 2009), our research team was interested in their use to foster more active communications between the students and their instructors, as well as to improve contact and collaboration among students, when the students are out in the field. We thought that nursing students would especially feel more need for communication at their community placements, such as clinics and patients' homes than when in hospitals. However, when asked if they used the mobile devices for communicating with instructors or fellow students, our participants indicated that, for the most part, they did not (See Table 5). This is consistent with the low volume of data downloading reported previously.
The figures in parentheses in Table 5 show the number of responses made by the three students in community placements. Only one student actively used the phone and text messaging to communicate with fellow students, implying that these students did not need to communicate any more regularly than students in hospital placements. In their interviews, these participants reaffirmed this, but the reason surprised our instructors and highlighted a problem with these placements.
Table 5. Usefulness for Enabling Communications.
Purpose |
Never |
1-2 Times |
3-4 Times |
5-6 Times |
> 10 |
Communicating With Other Students |
|||||
| Telephone | 5 (1) |
4 (1) |
0 |
1 |
2 (1) |
9 (2) |
1 (1) |
0 |
1 |
1 |
|
| Text Messaging | 7 (1) |
3 (2) |
0 |
1 |
1 |
| Audio Messaging | 12 (3) |
0 |
0 |
0 |
0 |
| Total | 33 |
8 |
0 |
3 |
4 |
| Percentage | 68.8 |
16.7 |
0.0 |
6.3 |
8.3 |
Communicating With Instructors |
|||||
| Telephone | 4 |
6 (2) |
1 |
0 |
1 (1) |
4 (1) |
6 (1) |
1 (1) |
1 |
0 |
|
| Text Messaging | 2 |
5 (1) |
3 (1) |
1 |
1 (1) |
| Audio Messaging | 12 (3) |
0 |
0 |
0 |
0 |
| Total | 22 |
17 |
5 |
2 |
2 |
| Percentage | 45.8 |
35.4 |
10.4 |
4.2 |
4.2 |
Students in the community placements tended to be constrained to passive, observational roles, rather than engaged in direct nursing care. They were not involved in making decisions about the care of patients and felt no need to seek the support and advice of their instructors or fellow students. A comment by Joan highlights this circumstance:
I'm sure… I mean I can totally see in the hospital how it would be really very valuable having that right beside you at the bedside. I mean I guess I don't see it as valuable because I didn't need to access information right on the spot and use it when I was in clients' home when we went on home visits and stuff like that. Because the information that they give people, it's all in pre-packaged, kind of a package that we give people for home visits, for baby visits and stuff. And anything that we're needing to record there, it has their preset type of sheet that they have.
Interaction Learning —The Learner in Context
The Interaction Learning intersection focuses on the social interaction that social technology enables. In the context of this study, not all the applications provided would normally be viewed as social technology. For instance, both the nursing programs and Mobile Office would seem to be standalone resource or productivity programs. However, in some situations, even these applications could serve a social purpose. For instance, as discussed below, the nursing software could be used directly when explaining a medication to patients or for teaching them about the management of their condition.
Overall, our participants reported divided opinions about whether the use of mobile devices in this specific practice experience was useful in support their learning. This course was brief (5 weeks) and the students were quite busy. Table 6 reports the mobile group's post-survey responses pertaining to the usefulness of the mobile applications in their practice experiences. The applications rated most useful were, in descending order, the nursing programs (drug reference and lab values), the mobile telephone and Pocket MSWord (tied for second), email (third) and browsing the Internet (fourth).
Table 6. Usefulness for Completing Course Learning Activities.
Application |
Useless |
Rarely Useful |
Sometimes Useful |
Frequently Useful |
N |
| Telephone | 2 |
3 |
2 |
5 |
12 |
3 |
2 |
5 |
2 |
12 |
|
| Browsing Internet | 2 |
4 |
1 |
5 |
12 |
| Text Messaging | 4 |
3 |
3 |
2 |
12 |
| Audio Messaging | 8 |
3 |
1 |
0 |
12 |
| Pocket Word | 2 |
3 |
3 |
4 |
12 |
| Pocket Excel | 7 |
2 |
2 |
0 |
11 |
| Nursing Software | 1 |
2 |
4 |
5 |
12 |
Note: One participant omitted the question about the use of Excel in this part of the survey.
In the interviews, our participants also reported the nursing software (2007 Lippincott's Nursing Drug Guide and Davis's Lab and Diagnostic Tests) as the most user-friendly and the program they used most in the trial. As well, they found Pocket Word simple to use, since it was not the full-blown desktop computer version. When asked which programs she found easiest to use, Alice commented:
Alice: Both. Drug guide, the drug manual and the… um, procedures…
Interviewer: Mmhmm.
Alice: …the procedures. And the Microsoft Word was actually really easy to create a Word document. And I'm technologically challenged, so if I can do it, anyone can do it! <laughs>
When asked about their specific use of the mobile applications, 8 mobile group participants indicated they used the Nursing programs at the bedside to verify information at least 5 times and 7 used these programs more than 10 times during their practice experience. However, only 2 participants reported using this information directly with patients and only one did so more than five times.
The participants also indicated in the interviews that they found the drug reference and lab values software the most useful application. When asked how she might use mobile devices in her overall Nursing education, Alice commented:
Um… well for anything that I've just mentioned, for… looking up… Um the biggest thing for any student, I would say, is looking up medications that you're unfamiliar with. Looking at the weights for, um, complex procedures like blood transfusions, that's right at your finger tips and it's accurate and up to date. Um, plasma transfusions, um, like compatibility of IV fluids and stuff, um…
This response highlights the fact that nine of the 12 mobile group members were in hospital placements, while only three were in community placements. Students in the hospitals would have been much more likely to give medications on a daily basis and, therefore, more inclined to verify drug information.
While our participants did not use the mobile applications regularly in their interactions with patients, there was some evidence that the iPAQs caught the attention of the nursing staff and served to help establish positive relationships between preceptors and students. For instance, Terrie noted that:
But again, she [preceptor] was very uncomfortable on computers and that sort of thing, so she just thought, you know, it's just another toy type thing. But um, my use of it in practice, they could see how quick I could access information on things too right? So that was… like… a positive, positively received by people because you're standing right there… and plus I would find questions for other people on the floor, and they didn't have to look them up in long, detailed textbooks and such, so they liked that part. So that part was received well.
Mobile Learning — FRAME Unfulfilled
In past work (Kenny et al., 2009), we pointed out that the delivery of nursing education requires physical mobility throughout the community and does not lend itself to direct teaching supervision models. We asked if m-learning, as represented by the FRAME model (Koole, 2009), could be implemented and sustained in independent nursing practice education settings. In the FRAME model, m-learning is defined as the overall intersection of the primary intersections: Device Usability, Social Technology and Interaction Learning. Each must be present to some degree for m-learning to have occurred. Figure 2 presents the outcomes of our study in the context of the FRAME model and demonstrates both the possibilities and problems for implementing m-learning in this context.
The results show that our participants believed that the use of mobile devices in practice education is both possible and desirable from a device usability perspective. Despite having to learn a number of features to use the iPAQs effectively, they reported them to be easy to learn and master overall. They found the devices to be readily portable and the screen sufficiently large for many uses and reported the nursing software (drug reference and lab values) and familiar programs such as Pocket Word simple to learn and to use at the point-of-care.
However, despite direct teaching and practice during the orientation, few of our students were able to make effective use of GPRS data connectivity when using the devices on their own. This is likely related to the pilot nature of the experience. Faced with an intensive, one-month, practice experience, the students did not have much time to fully master the devices. This was compounded by the fact that the devices did not belong to the students nor did they have them for an extended period of time. As a result, they did not devote the necessary time and energy to fully integrating them into their learning.
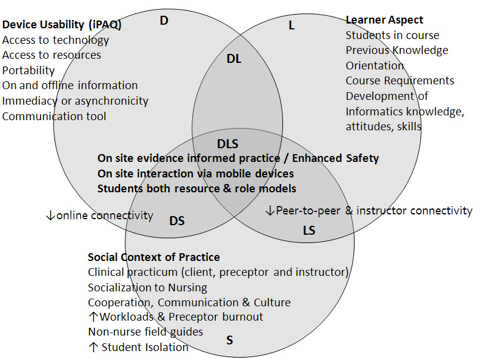
Figure 2. M-learning in the nursing practice education context.
The Social Technology intersection describes how mobile devices enable communication and collaboration. Our participants did not find the mobile devices useful for communication purposes, despite the inclusion of local cell phone service. They encountered a hospital culture and policies that precluded the use of wireless devices in those settings and also had difficulty with connectivity. The most serious impediment was the inability to use the iPAQs to access the course website, the main vehicle for both accessing course documents and for posting messages to the instructors and other students. It is not clear, therefore, from this pilot study that m-learning in the context of nursing practice education can enable communication and collaboration among instructors and students, or if the use of mobile devices can effectively support the distance components of a blended learning course of this sort.
Finally, the Interaction Learning intersection focuses on the social interaction enabled by social technology. Our results appear to indicate that m-learning is useful from this perspective to a certain extent. Our participants referred to the referencing nursing software as the most useful feature of the mobile devices for their nursing practice experiences. They found the devices convenient for immediate reference and easy to access when needed. This software was not designed to enable direct person-to-person interaction, but did so indirectly either through patient teaching or by fostering dialogue between the students and their supervising nurses.
In conclusion, our study confirmed that the use of m-learning, at least with mobile devices providing the breadth of features afforded by the HP iPAQ, is feasible in actual nursing practice education settings. At a minimum, mobile devices have the potential to be very effective in allowing students and instructors ready access to resources at the point-of-care. We have not yet been able to determine if the interactive and communication uses of mobile devices can be used in this setting. This should be more thoroughly investigated in future investigations.
Future Research
Our participants' failure to fully learn and use the mobile devices can be attributed in part to the voluntary, pilot nature of the experience and in part to insufficient time to focus on learning the devices or to use them fully in their learning during an intensive, one-month, practice experience. This highlights the need for a more extensive, real-life trial of m-learning, one in which the use of mobile devices is an integral part of a course or even a complete program. Students should be supplied with, or asked to acquire, their own mobile devices and the use of these devices in the course or program made mandatory.
In addition, research on m-learning needs to move beyond descriptive studies and to focus on a more theoretical basis for its implementation and use. One of the initial interests of our research group in choosing to study the use of mobile learning in nursing practice education was our belief that mobile technology could facilitate learning in this context by assisting instructor-student and student-student communication. While the FRAME model proved useful in our analysis of m-learning in this context, it is a new model and not well supported by empirical research. It may be more fruitful in future to consider the application to m-learning in this context of an established theory such as the Community of Inquiry (COI) model (Garrison, Anderson, & Archer, 2000).
The COI model assumes that learning occurs within the community through the interaction of three core elements: cognitive presence, social presence, and teaching presence. We are interested in determining in particular how improved communication might help to build and maintain learning community by increasing learners' cognitive presence and teaching presence. We also believe that the COI and FRAME (Koole, 2006, 2009) models have considerable overlap, with the latter likely describing a subset of the former specific to m-learning, and intend to investigate further this relationship.
1. Pseudonyms are used in place of participants' actual names.
Cahoon, J. (2002, April). Handhelds in health care: Benefits of content at the point of care. Advances in Clinical Knowledge Management, 5. Retrieved January 26, 2009, from:
http://www.openclinical.org/docs/ext/workshops/ackm5/absCahoon.pdf
Davenport, C. (2004). Analysis of PDAs in nursing: Benefits and barriers. Retrieved January 26, 2009, from:
Garrison, D. R., Anderson, T., & Archer, W. (2000). Critical inquiry in a text-based environment: Computer conferencing in higher education. The Internet and Higher Education, 2(2-3), 87-105.
Garrison, D.R., & Kanuka, H. (2004). Blended learning: Uncovering its transformative potential in higher education. Internet and Higher Education 7(2), 95-105.
Goldsworthy, S., Lawrence, N., & Goodman, W. (2006). The use of Personal Digital Assistants at the point of care in an undergraduate nursing program [Electronic version]. CIN, 24(3), 138-143.
Keegan, D. (1996). Foundations of distance education (3rd ed.). London: Routledge.
Kenny, R.F., Park, C.L., Van Neste-Kenny, J.M.C., Burton, P.A. & Meiers, J. (2008). The feasibility of using mobile devices in nursing practice education. In J. Traxler, B. Riorden & C. Dennett (Eds.), Proceedings of mLearn 2008, the 7th World Conference on Mobile Learning, Shropshire, England.
Kenny, R.F., Park, C., Van Neste-Kenny, J.M.C., Burton, P.A. & Meiers, J. (2009). Using mobile learning to enhance the quality of nursing practice education. In M. Ally (Ed.), Mobile learning: Transforming the delivery of education and training. Athabasca, AB: Athabasca University Press.
Koole, M. L. (2005). The framework for the rational analysis of mobile education (FRAME) model: An evaluation of mobile devices for distance education. Unpublished master's thesis. Athabasca University, Alberta. Available from: http://library.athabascau.ca/drr/viewdtr.php?course=thes&id=205
Koole, M. L. (2009). A model for framing mobile learning. In M. Ally (Ed.), Mobile learning: Transforming the delivery of education and training. Athabasca, AB: Athabasca University Press.
Koole, M. L., & Ally, M. (2006, April). Framework for the rational analysis of mobile education (FRAME) model: Revising the ABCs of educational practices. Networking International Conference on Systems and International Conference on Mobile Communications and Learning Technologies, 216-216.
Kukulska-Hulme, A., & Traxler, J. (2005). Mobile teaching and learning. In A. Kukulska-Hulme, A. & J. Traxler (Eds.). Mobile learning: A handbook for educators and trainers (pp. 25-44). London: Routledge.
Lehman, K. (2003). Clinical nursing instructors' use of handheld computers for student recordkeeping [Electronic version]. Journal of Nursing Education, 42(10), 41-42.
Miller, J., Shaw-Kokot, J. R., Arnold, M. S., Boggin, T., Crowell, K. E., Allehri, F., et al. (2005). A study of personal digital assistants to enhance undergraduate clinical nursing education. Journal of Nursing Education, 44, 19-26.
Newbolt, S. K. (2003, October). New uses for wireless technology. Nursing Management, 22, 22-32.
Park, C. (2006). [Survey data on mobile use by Nurse Practitioner students]. Unpublished raw data.
Rosenthal, K. (2003). "Touch" vs. "tech": Valuing nursing specific PDA software. Nursing Management, 34(7), 58.
Stroud, S.D., Erkel, E.A., & Smith, C.A. (2005). The use of Personal Digital Assistants by Nurse Practitioner students and faculty [Electronic version]. Journal of the American Academy of Nurse Practitioners, 17(2), 67-75.
Traxler, J. (2007). Defining, discussing and evaluating mobile learning: The moving finger writes and having writ. The International Review of Research in Open and Distance Learning, 8(2). Available from:
Villeneuve, M., & MacDonald, J. (2006). Toward 2020: Visions for nursing. Ottawa, ON: Canadian Nurses Association.
Richard F. Kenny is an Associate Professor with the Center for Distance Education at Athabasca University, where he teaches instructional design and learning theory. His research interests include instructional design and change agency, emerging technologies to foster higher-order thinking, and mobile learning applications and strategies. E-mail: rickk@athabascau.ca
Jocelyne M. C. Van Neste-Kenny is the Dean of Health, Human Services and Applied Business Technology at North Island College in Courtenay, British Columbia, Canada. Her research interests include practice education models, emerging technologies in practice education, and interprofessional education. E-mail: jvannest@nic.bc.ca
Caroline Park is an Associate Professor with the Centre for Nursing and Health Studies at Athabasca University, where she teaches in the Masters of Health Studies and the Masters of Nursing programs. Besides an interest in hand held devices for learning, she is participating in research relating to inter-disciplinary research teams.
E-mail: clpark@athabascau.ca
Pamela A. Burton is an instructor with the Collaboration for Academic Education in Nursing Program (Bachelor of Science in Nursing) at North Island College in Courtenay, British Columbia, Canada. Her research interests include the use of mobile technologies in nursing education and prevention of medication errors. E-mail: Pam.Burton@nic.bc.ca
Jan Meiers is an instructor with the Collaboration for Academic Education in Nursing Program (Bachelor of Science in Nursing) at North Island College in Courtenay, British Columbia, Canada. Her research interests include the use of mobile technologies in nursing education and student attrition in BSN education programs.
E-mail: Jan.Meiers@nic.bc.ca